I thought to begin today's post by coining a term -- "civilicide" -- or a civilization deliberately causing its own demise. But a Google search immediately turned up a familiar name -- Dr. Terry Collins -- who coined it in an earlier article on whether or not a technologically advanced society can survive on this planet. In that article describing a course in green chemistry and sustainable societies at Carnegie Mellon, where he teaches, he claims that "A civilization that does not conceive of itself as a living entity embodying a past from which it can learn, a present in which it chooses to act for the common good, and a future of which the open-ended good is its dominant strategic objective is doomed to drift helmless toward self destruction." He decries academic participation in civilicide in the Faustian bargains it often makes with industry for funding. Instead, he implores readers -- scientists and leaders -- to move us towards "Yes." We can achieve sustainability in our day. As in my conversation with him in this forum, he argues that we need a new ethics more fitted to the current ecological crisis.
I independently arrived at "civilicide" this week as I witnessed the brutal undoing of the very meager and insufficient protections we have previously had through the EPA. As with the destruction of many of our most important institutions, those committing these crimes against humanity are both transparently ignorant and openly malicious in their vandalism. It is unforgivable that the EPA website now touts the rollback of regulations on coal, oil, and gas as "Unleashing American Energy," as if widespread renewables could not have done the same without supercharging the climate change that is already wreaking havoc right here in the US of A.
EPA administrator Lee Zeldin talks about lowering costs for American families by allowing emissions of mercury, air pollution, and many other pollutants to soar unfettered. You know what does NOT lower costs for Americans? A child with cancer, ADHD, autism, diabetes, depression, or other environmentally-linked illness. A child with a lower IQ, whose lifetime earnings will measurably decrease. We are not talking about one child here and another there. We are talking about ALL children, to one degree or another.
MAGA seems motivated by the idea that cruelty to the most vulnerable, including our own children, is the swiftest way to greater prosperity, even though we are already prosperous, even though so much evidence suggests that humans, like most other organisms on Earth, have succeeded more through cooperation and mutualism than through competition, red in tooth and claw. As Potawatomi botanist Robin Wall Kimmerer reminds us, "all flourishing is mutual." We have attacked our nearest allies for benefits we easily could have obtained by asking nicely.
I contemplated our current civilicide as I read Sharon Lerner's brilliant latest, on the challenges to the Biden-era ban on TCE (trichloroethylene), a notorious chemical used to dry-clean clothes or dissolve oil on machinery, which has been conclusively linked to cancer, Parkinson's, organ damage, and heart defects in babies. The victims Lerner interviewed, doomed to an early demise from Parkinson's, had hoped that at least their children and grandchildren would be protected. Now, that is unlikely.
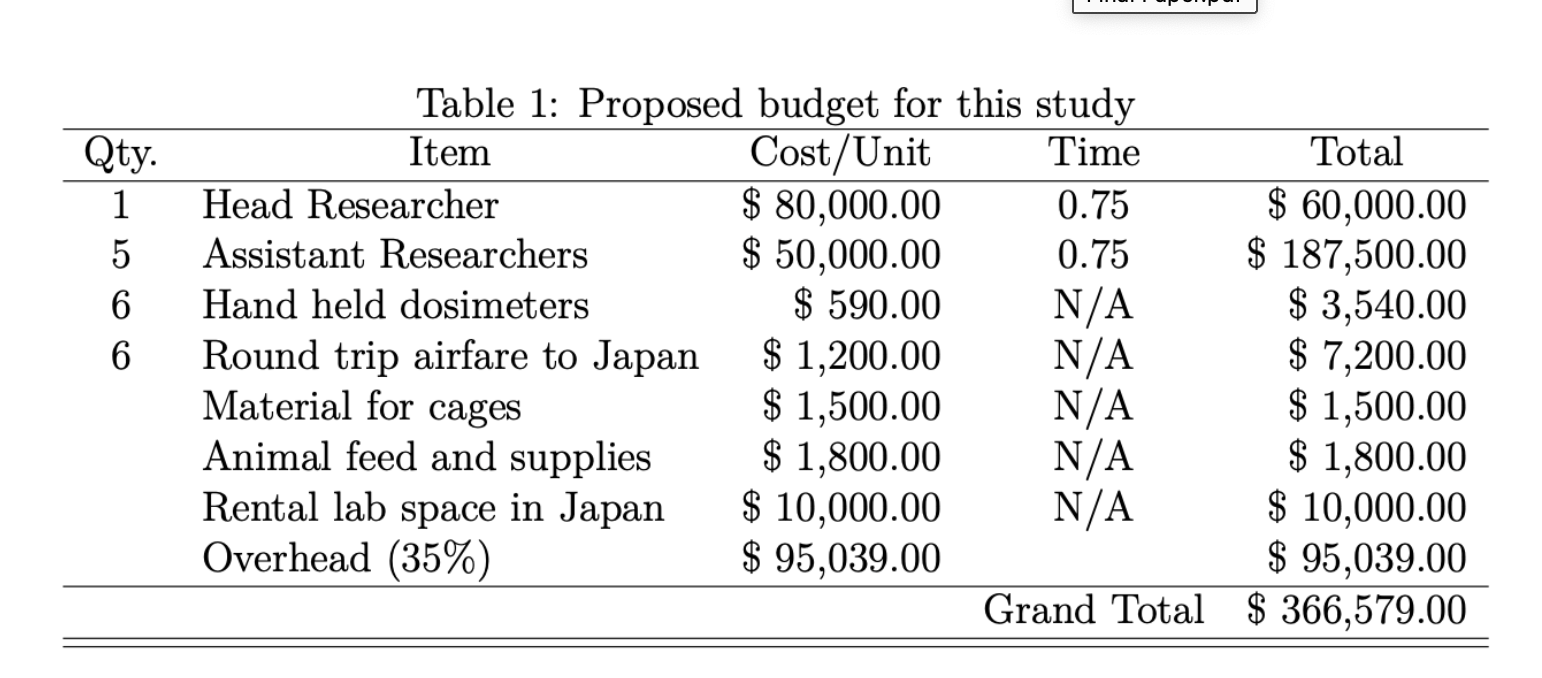
Why tragic? If the death of many humans and all the fruits of civilization that make life comfortable and happy for so many were not enough, we may be facing the end of the planet as we know it, having squandered a last opportunity to change our ways and lead the world by saving it. A superpower unleashed, undemocratic, uncaring, unmoored from its origins, and absolutely, incontrovertibly unethical will only hasten our demise. The USA today is much more able to recklessly destroy the world than was 1938 Germany. All of this is tragic because, as Jim Hansen said in 2016, it is completely unnecessary. We already have the tools; we already have the solutions. We could do it on budget. All we lack is the culture and the political will. That, it turns out, is no small thing, as Mark Jacobson and Mark Delucchi pronounced in a brilliant series of articles delineating these solutions.
I hardly know what to say. Many of the scientists and activists I know are teetering on despair. And yet, despair cannot be an option. In the face of evil, under an onslaught of incipient autocracy, what can we do? We can still protest, which is what I intend to do this weekend. I will be in Bloomington, Illinois, but I hope to join you all -- at least in spirit.